
The concept of a ‘power triangle’ comes from the reflection that only through safety can we flourish and achieve our full potential (Maslow, 1954, Edmondson, 1999), having the confidence to participate, having autonomy over our lives, and therefore having power.
How to convey the complexity of Trauma Informed Practice.
I have worked within education for the past 20 years and, throughout that time, my passion for relational practice and supporting children has only grown. As a trainee Educational Psychologist, my doctoral research explored how mentalisation supports young people with Social, Emotional and Mental Health (SEMH) needs who have experienced adversity (Williams, 2023).
In 2024, I became a Specialist Educational Psychologist for the Virtual School. With this role came new opportunities to share ideas and support some of our most vulnerable young people. When asked to speak at a Trauma-Informed conference for Designated Teachers (and to summarise trauma-informed provision across primary and secondary phases in just 45 minutes), I faced a familiar challenge: the research base is vast, and teachers have limited time to digest it and – more importantly – implement ideas from it.
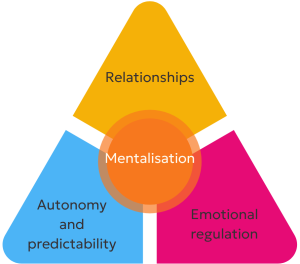
My response was to create something simple, practical, and grounded in evidence: The Safety Power Triangle.
This framework brings together three core components of trauma-informed provision:
- relationships
- emotional regulation
- and autonomy/predictability
This focus was designed to help schools reflect on what they already do well and where they can strengthen their support.
Why mentalisation must come first
Before considering any provision for a young person, I believe it is important to engage in mentalisation. Mentalisation is the imaginative process that allows us to think about the thoughts and behaviours of ourselves and others (Allen & Fonagy, 2006), as well as their goals, intentions, and emotions (Bateman & Fonagy, 2013).
When mentalisation occurs and is responded to, relationships and attachments are strengthened and needs are met (Slade, Grienenberger, Bernbach, Levy & Locker, 2005). When considering the young people we work with in educational settings, the mental effort to interpret their behaviours by thinking about their thinking can lead to adaptations in the way they are supported, through adults shaping provision to meet their needs (Williams, 2023). This means that mentalisation can facilitate more personalised provision for a young person, helping them to be better understood, have their needs met (Williams, 2023), and feel a greater sense of safety.
Reflection question for settings – How do you interpret the intentions, goals, and behaviour of the young people you are working with?
Working from a hopeful standpoint, it is important to believe in the impact that the right provision can have on our young people. Making adaptations through provision allows us to consider what can be changed and adjusted in the environment, as opposed to adopting a child-deficit model and thinking about what needs to be changed within the child. The Safety Power Triangle allows for reflection on the support currently in place and consideration of new provision ideas.
Understanding Trauma-Informed Practice
Trauma-informed practice recognises that trauma affects development at social, biological, neurological, and psychological levels. It aims to increase awareness of how trauma impacts a child’s ability to feel safe and build relationships (Department for Education, 2023).
While some narratives focus heavily on brain-based explanations, Billington (2017) warns that this can unintentionally reinforce a medical model that places the “problem” within the child.
More recent models, such as the Neurocognitive Social Transactional Model (NSTM) (McCrory, Foulkes & Viding, 2022), emphasise the bidirectional relationship between a child and their environment.
Trauma can create neurocognitive adaptations that impact a child’s social behaviour, which in turn affects how others respond to them, creating a social environment that can increase risk. This occurs through social thinning (a reduction in the quality and number of relationships) and an increase in interpersonal stressors.
The transactional nature of this theory helps us to look beyond the individual and consider their wider social world and interactions within it. It considers that timely intervention and opportunities can reverse social thinning and decrease stress generation, promoting positive outcomes for young people through building positive relationships and environments (McCrory, Foulkes, & Viding, 2022). This research demonstrates how provision and intervention are essential in supporting young people who have experienced trauma to flourish and thrive.
The Safety Power Triangle
The idea of the Safety Power Triangle came from the view that being trauma-informed must involve creating an ethos and culture around feeling safe. Through reflection with colleagues, three themes consistently emerged when discussing what helps people feel safe:
- Being with trusted, caring people
- Being in a predictable environment
- Feeling calm and emotionally supported
These became the three points of the Safety Power Triangle:
- Strong relationships
- Emotional regulation and co-regulation
- Autonomy and predictability
Following these informal discussions and reflections, I set out to consider theoretically why these three points of the triangle may support trauma-informed provision and a sense of safety.
The safety power triangle framework synthesises existing research into a simple, accessible tool for schools to use when planning or reviewing trauma-informed provision.
Reflection question: When do you feel safe?
Relationships: the foundation of safety
The evidence is clear that strong relationships between children and school staff are linked to improved academic, social, and emotional outcomes (Michael & Frederickson, 2013; Lloyd & O’Regan, 1999; Hattie, 2009).
For children who have experienced trauma, relationships are not just helpful, they are healing. Perry (2017) puts it simply: “People, not programs, change people.”
Applying this to the school setting, Bomber (2008) introduced the concept of the ‘key adult’ within an educational setting and how they work to support children. The key adult role is designed to support children who may have experienced trauma or have attachment differences. Bomber (2008) shares that staff should take on the role of an additional attachment figure or safe adult with whom the child can have a meaningful relationship.
This special relationship can facilitate ‘second chance learning’ and provide an alternative to the child’s internal working model, which may be negative about the world and the self, due to trauma or life experience (Bomber, 2008). Geddes (2006) also shares that, although patterns of attachment can be created in early childhood, they can also be shaped later by important relationships, which can ameliorate earlier adverse experiences.
The main aim of the key adult relationship is to be attuned to a child and build relative dependency — becoming a person who meets their needs and on whom they can depend (Bomber, 2008) — and therefore a ‘safe’ adult.
Reflection question for settings – How do you promote the building of relationships for young people?
Emotional regulation and co-regulation
Although emotional regulation can be seen as something intrinsic, a wide body of evidence suggests that emotional regulation must be modelled, taught, and done with a child through provision and co-regulation with an adult (Siegel & Bryson, 2011, Gottman & DeClaire, 1997). Supporting children to manage their emotions has a positive impact when considering the bidirectional nature of the NSTM (McCrory et al., 2022): children who are supported to learn how to manage stress and emotions are less likely to struggle with interpersonal relationships and conflict.
Gerhardt (2004), suggests that emotional “immunity” comes from early experiences of being securely held, physically comforted, recognised, and guided through recovery from stress.
For some trauma-experienced children, self-regulation is difficult because they struggle to differentiate between feelings and bodily sensations and do not know how to move between different states or recognise that they need to (Bomber, 2007). To develop these skills, children need the experience of an adult who provides sensitive care, contains their emotional needs, and reflects and comments on what is happening to them emotionally to help them make sense of it (Bomber, 2007). Before we can self-regulate, we need someone alongside us providing feedback and insights into our thoughts and feelings—this is the foundation of emotional literacy.
As well as building emotional literacy through co-regulation, using mentalisation to explore what children’s behaviours might be communicating and what their ‘triggers’ might be can help us meet their needs and work proactively. Andrews (2023) shares that, by noticing and responding when children begin to become heightened, and intervening at that point, we can work proactively to avoid moments of dysregulation and support the child to recognise when they are becoming heightened.
Reflection questions for settings – How do you promote the development of emotional regulation skills? What strategies do you have to support young people who are beginning to become heightened?
Autonomy and predictability
Although these two concepts may be distinct and separate, when considering them through the lens of trauma-informed provision, I perceive them as interrelated. This is because a sense of autonomy and choice can create a sense of predictability in one’s own life.
Trauma-experienced young people can struggle with unpredictability in educational settings, which can lead to stress responses (Bekker & Bekker, 2025). Therefore, children and young people need learning environments where they know what to expect in order to feel safe. Educational settings should create clear expectations to promote a feeling of stability (Bekker & Bekker, 2025).
Self Determination Theory (SDT) suggests that humans grow, thrive, experience increased wellbeing, and achieve goals when their basic human needs are fulfilled (Ryan & Deci, 2000). These needs are relatedness, mastery, and autonomy. SDT explains that autonomy is key to human motivation. For many young people who have experienced trauma, it could be said that their human needs have not been met and their choices have been taken away (i.e, their autonomy has been reduced). Mancini (2008) suggests that autonomy is the cornerstone of SDT when considering recovery from trauma, because autonomy is essential for motivation (an important component of wellbeing), and this is often diminished when people are struggling with their wellbeing. Therefore, helping young people to have choices in their day, and to anticipate what is happening next, should support their sense of safety.
Reflection question for settings – How do you promote choices and increase a sense of predictability for young people?
Closing comments
The Safety Power Triangle does not introduce new concepts, instead it brings together well-established ideas into a clear, practical framework that schools can use to strengthen trauma-informed provision when time is scarce.
Sharing the three points of the triangle with an educational professional provides a framework for thinking about how to create safety, while allowing them to bring in their own ideas that they know they can resource in their setting. This also creates a sense of autonomy, as when people generate ideas themselves, this satisfies the psychological need for autonomy (Ryan & Deci, 2000).
References
Allen, J. G., & Fonagy, P. (Eds.). (2006). The handbook of mentalization-based treatment. John Wiley & Sons.
Andrews, H (2023) Green with moments in amber. In Morgan, F., & Costello, E. (2023). Square Pegs: Inclusivity, compassion and fitting in-a guide for schools. Crown House Publishing Ltd.
Bateman, A. and Fonagy, P. (2013) Mentalization-Based Treatment, Psychoanalytic Inquiry, 33:6, 595-613, DOI: 10.1080/07351690.2013.835170.
Bekker, T., & Bekker, S. (2025). The neuropsychology of trauma-exposed children: Implications for inclusive teaching and learning. International Journal of Inclusive Education. Advance online publication. https://doi.org/10.1080/13603116.2025.2555394 (doi.org in Bing)
Billington, T. (2017). Educational inclusion and critical neuroscience: friends or foes? International Journal of Inclusive Education, 21(8), 866–880. https://doi.org/10.1080/13603116.2017.1283717
Bomber, L. M. (2007). Inside I’m hurting: Practical strategies for supporting children with attachment difficulties in schools. Worth Publishing.
Deci, E. L. & Ryan, R. M. (2000). Intrinsic and extrinsic motivations: Classic definitions and new directions. Contemporary Educational Psychology, 25(1), 54–67.
https://doi.org/10.1006/ceps.1999.1020
Department for Education. (2023). Working definition of trauma-informed practice. UK Government. https://www.gov.uk/government/publications/working-definition-of-trauma-informed-practice/working-definition-of-trauma-informed-practice
Edmondson, A. (1999). Psychological safety and learning behavior in work teams. Administrative Science Quarterly, 44(2), 350–383
Geddes, H. (2006) Attachment in the Classroom. London: Worth Publishing.
Gerhardt, S. (2004). Why Love Matters: How Affection Shapes a Baby’s Brain. Routledge. First published 2004, London
Gottman, J., & DeClaire, J. (1997). Raising an emotionally intelligent child. Simon & Schuster.
Hattie, J. (2009). Visible learning: A synthesis of over 800 meta-analyses relating to achievement. London: Routledge.
Lloyd, G., and A. O’Regan (1999). “Education for Social Exclusion? Issues to Do with the Effectiveness of Educational Provision for Young Women with ‘Social, Emotional and Behavioural Difficulties’.” Emotional and Behavioural Difficulties 4 (2): 38–46.
Mancini, A. D. (2008). Self-determination theory: A framework for the recovery paradigm. Advances in Psychiatric Treatment, 14(5), 358-365.
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50(4), 370–396
McCrory, E., Foulkes, L., & Viding, E. (2022). Social thinning and stress generation after childhood maltreatment: A neurocognitive social transactional model of psychiatric vulnerability. The Lancet Psychiatry, 9(10), 828-837.
Michael, S., & Frederickson, N. (2013). Improving pupil referral unit outcomes: pupil perspectives. Emotional and Behavioural Difficulties, 18(4), 407–422. https://doi.org/10.1080/13632752.2013.801112
Perry, B. D. (2017). The boy who was raised as a dog: And other stories from a child psychiatrist’s notebook (Rev. ed.). Basic Books.
Siegel, D. J., & Bryson, T. P. (2011). The whole-brain child: 12 revolutionary strategies to nurture your child’s developing mind. Delacorte Press.
Slade, A. Grienenberger, J. Bernbach, E., Levy, D. and Locker, A. (2005). Maternal reflective functioning, attachment, and the transmission gap: A preliminary study. Attachment and Human Development, 7, 283-98.
Williams, Emily (2023). “It’s like reading and responding”: An exploration of the appearance and functioning of mentalising in the relationship between key adults and young people with Social Emotional and Mental Health needs in the primary school setting. DEdCPsy thesis, University of Sheffield